

Summer months are beleaguered by their own set of infections/diseases. Heatstroke, food poisoning, eye infection, mumps, measles, chickenpox, flu, asthma attacks… the list goes on. An uptick in the disease-causing pathogens, unhealthy eating and sleeping habits, pollution, poor sanitation, and subsequent lowered immunity cause them to culminate.
Typhoid is one of them. Also called enteric fever, it is an infectious disease occurring in the intestinal tract and occasionally, in the bloodstream. It is caused by Salmonella typhi – a motile, rod-shaped gram-negative bacteria.
 Typhoid fever is a major health menace in poor and developing Asian countries (India, Pakistan, Sri Lanka, and Bangladesh), Africa and Latin America; principally owing to the consumption of unsafe drinking water, inadequate sewage disposal and flooding. Travelers to the endemic areas of these countries stand a greater risk of the infection.
Typhoid fever is a major health menace in poor and developing Asian countries (India, Pakistan, Sri Lanka, and Bangladesh), Africa and Latin America; principally owing to the consumption of unsafe drinking water, inadequate sewage disposal and flooding. Travelers to the endemic areas of these countries stand a greater risk of the infection.
Typhoid fever has no age limit. It can affect women, men, and children of all ages.
Typhoid is a disease of humans – it has only humans as ‘cases’ or ‘carriers’. There are no animal reservoirs of S Typhi.
The disease and how it affects you
In nature, S Typhi live in the gut of infected humans and are passed out in their feces and urine. People become infected after eating/drinking foods or beverages handled by an infected person or by drinking water that has been contaminated by sewage containing the bacteria.
Salmonella bacterium can live in water or dried up sewage for weeks.
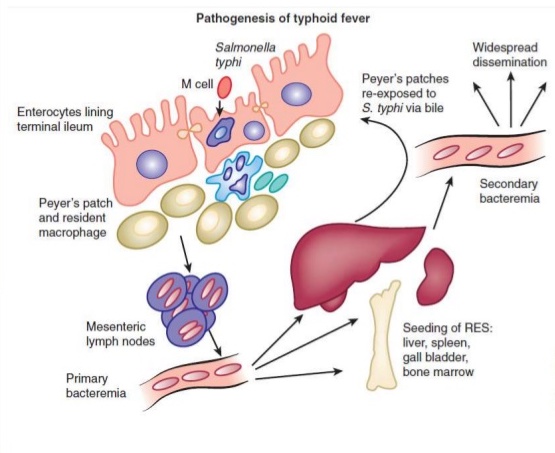 After ingestion, the bacteria enter the gut to invade the small intestines and enter the bloodstream temporarily. They are then carried by your white blood cells (WBCs) to the liver, spleen, and bone marrow. The bacteria multiply in the cells of these organs to re-enter the bloodstream.
After ingestion, the bacteria enter the gut to invade the small intestines and enter the bloodstream temporarily. They are then carried by your white blood cells (WBCs) to the liver, spleen, and bone marrow. The bacteria multiply in the cells of these organs to re-enter the bloodstream.
You develop symptoms, including fever, when the organism re-enters your bloodstream.
Bacteria then invade the gallbladder, biliary system, and the lymphatic tissue of the bowel (Peyer’s patches), where they multiply in high numbers. The bacteria pass back into the intestinal tract and can be identified for diagnosis in stool cultures.
Stool cultures are sensitive in the early and late stages of the disease but often must be supplemented with blood cultures to make a definite diagnosis.
How does the infection spread?
The disease is contagious i.e. it can spread between individuals when an infected person passes out the bacteria in their feces. Though typhoid is majorly a water and foodborne disease, it can also spread through close contact with an infected person.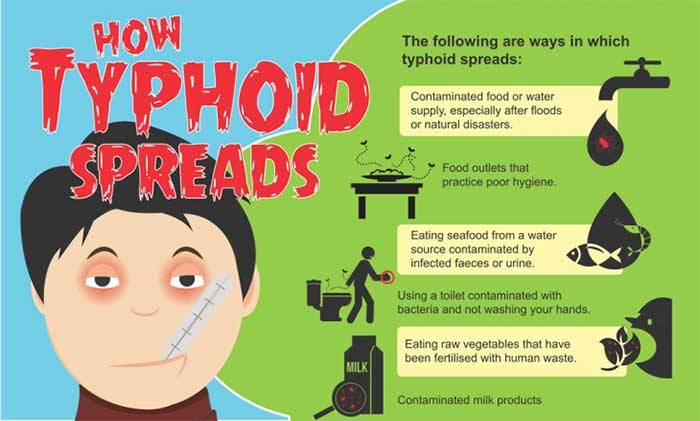
Feco-oral-route
- Eating or drinking food/beverages that have been handled by a person who is shedding S. Typhi in stools or urine.
- By consuming sewage-contaminated water for drinking or washing food.
- Insects like flies and cockroaches can spread the infection directly from stool to foods eaten up by us through an indirect host-host transmission.


Congenital by transplacental bacteremic mother to her fetus.
Intrapartum (during child-birth) only through a fecal-oral route from a carrier mother.
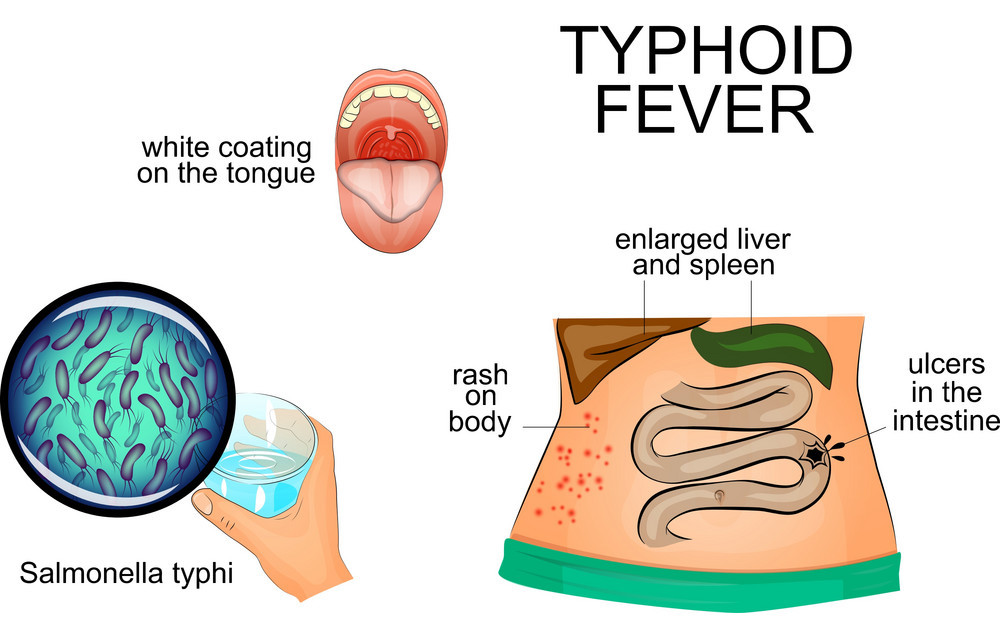
What are the Symptoms?
The symptoms of typhoid fever start 7-14 days after consuming food or drinks contaminated with the bacteria. They include high fever, abdominal pain, headache, constipation or diarrhea and ‘rose spots’ on the skin. Untreated typhoid runs a course having 4 classical stages each lasting for about a week.
The 1st week:
- Insidious onset of fever that rises in a ‘stepladder’ fashion.
- Headache, malaise, relatively slow heartbeat (bradycardia).
- Minimal nonproductive cough.
- There may be abdominal pain and episodes of bleeding from the nose.
Into the 2nd week of untreated infection, the symptoms are:
 Fever reaching and hovering around 40°C (104°F) with a relatively low pulse rate.
Fever reaching and hovering around 40°C (104°F) with a relatively low pulse rate.- Bloated abdomen with pain in the right lower quadrant. The bowel sounds are loud and audible.
- Minute ‘rose-colored spots’ over the skin of the lower chest and upper abdomen, occur in nearly 50% of cases and last for 3 to 5 days.
- The person may appear to be in a delirious state, constantly muttering to himself or picking at the bed-sheets.
- Constipation or diarrhea may occur. Around 5 to 8 diarrheic stools, greenish, looking like ‘pea-soup’ are seen.
- Joint pains may be present.
- Liver and spleen may get enlarged.
The 3rd week of untreated typhoid can present with life-threatening emergencies:
- Intestinal perforation – perforation of the walls of small intestine.
- Bleeding into the intestines
- Spread of the infection to the brain via the blood causing inflammation of the brain.
- Inflammation of the gall-bladder, heart muscles; infections in the bones, and formation of abscesses within other important internal organs.
There can be a relapse in 2-4% cases.
Carrier State:
About 3%-5% of sufferers become carriers of the bacteria after the acute illness is over. The bacteria continue to multiply in their gallbladder, bile ducts, or liver and they keep shedding the bacillus out of their bowels. Also, some people may suffer a very mild illness that goes unrecognized. They can become long-term carriers of the bacteria.
These chronic carriers may have no symptoms and can be the source of new outbreaks of typhoid fever for many years.
Diagnosis
Important changes in lab investigations are:
Complete Blood Count (CBC): In the first week of infection will show –
- Reduction in the total number of WBCs and eosinophils.
- Increased number of lymphocytes.
Blood Cultures are positive in the 1st and 2nd weeks of infection. They become rapidly negative on treatment with antibiotics. Stool, urine or bone marrow cultures are also positive.
Widal Test: Detects antibodies against the bacillus in the serum. This test is negative in the 1st week and becomes strongly positive from the 2nd week onwards. (titers of O-1/100, H-1/200 and more are significant)
Elisa: Typhidot, detects IgM and IgG antibodies against the outer membrane protein of S Typhi. This becomes positive within 2-3 days of infection but is not a quantitative test. The result is only positive or negative.
Liver Function Tests: From the second week onwards, the liver transaminases appear to be elevated.
Blood, stool, urine or bone marrow cultures are the most conclusive investigation to detect the presence of S Typhi.
Treatment
Typhoid, timely treated, is rarely fatal.
Use of broad-spectrum antibiotics (chloramphenicol, ampicillin, trimethoprim-sulfamethoxazole, and ciprofloxacin) have decreased the suffering in typhoid fever to a large extent, however, the use of fluoroquinolone and ciprofloxacin is reaching its limitations due to a developing drug resistance by the bacterium.
For those who develop complications like a perforation in the intestinal walls, surgical repair is indicated.
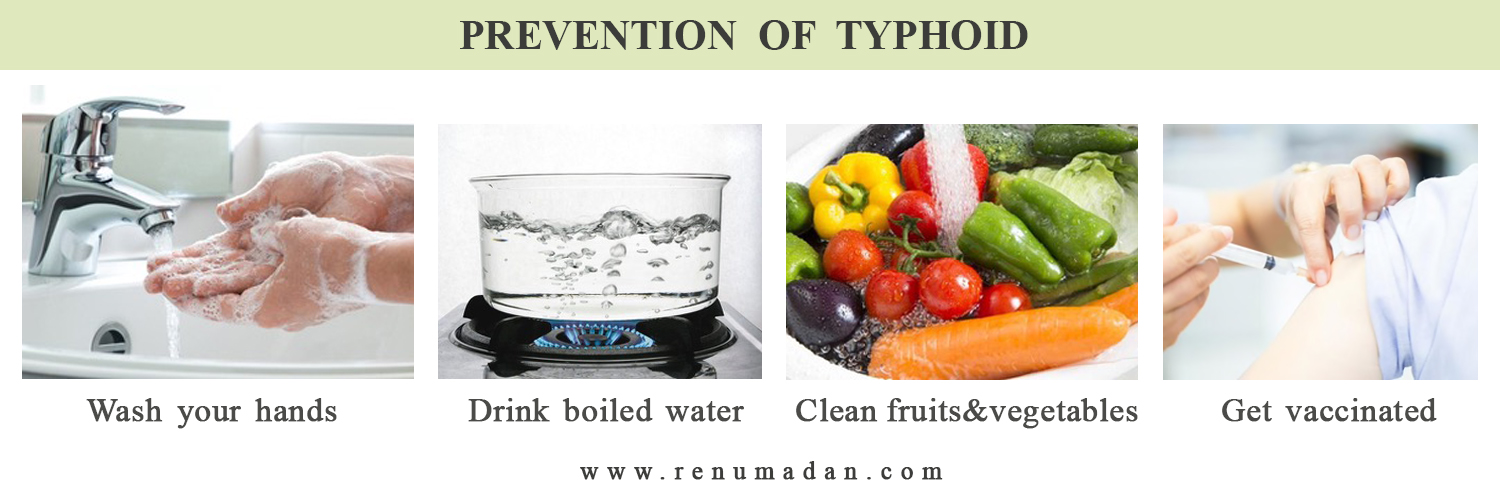
Prevention
# WHO recommends the use of vaccines and good hygiene practices as the two-prongs to control this disease and stop it from spreading.
For those traveling to high-risk areas, two kinds of vaccines are available:
- Inactivated typhoid vaccine (shot) – given at least 2 weeks before the travel as a single injection (more effective).
- Live typhoid vaccine (oral) – given as three capsules to take on alternate days. Usually not recommended for children under six and people with a weakened immune system as in HIV/AIDS, since the vaccine contains live attenuated(weakened) Salmonella typhi bacteria.
Booster vaccinations are recommended every 3 years if you continue to be at risk of infection.
There are also combined typhoid and hepatitis A injections available for people aged 15 or older.
# Following are some general hygiene rules to help minimize the chance of typhoid infection:
- Wash hands with soap & water as often as possible, esp. before eating/preparing food/after using the toilet.
- Avoid drinking untreated/contaminated water. Opt for bottled water when traveling.
- If bottled water cannot be sourced, ensure water is heated on a rolling boil for at least 1 minute before consuming.
- Do not have ice in drinks.
- Wash fruits & vegetables thoroughly before consuming.
- Avoid eating street/uncovered food.
- Choose hot food.
- Practice good sanitation habits.
Homoeopathic Medicines for Typhoid
Here are a few gems of Homoeopathy, that have been timelessly found effective in the various stages of Typhoid.
- Baptisia and Lachesis – for continuous fever with marked delirium and offensive discharges.
- Arsenic Album and Carbo Vegetabilis – when fever is accompanied with great prostration.
- Arnica and Rhus Tox – for acute body aches and restlessness with fever.
- Muriaticum Acidum and Bryonia Alba – are the top medicines for typhoid with abdominal symptoms – constipation or involuntary stools.
- Lachesis and Arsenic Album – are the remedies required if one develops bedsores. They facilitate the healing, help in wound drying, taking care of the pain and restlessness of the patient.
- Eucalyptus and Terebinthina — for typhoid with continuously rising fever and foul discharges – oral, rectal, urinary and from the bedsores.
A Holistic approach is followed in treating Typhoid patients successfully through Homoeopathy.
Note: The images used alogside text are taken from the net only for a descriptive purpose.
